
Bowl For a Cause - First MSF Bowling Challenge
Enjoy a philanthropy bowling evening to save lives
For over 50 years, Doctors Without Borders/Médecins Sans Frontières (MSF) a medical humanitarian organisation, has delivered life-saving care to people who have nowhere else to turn; fighting epidemics, war injuries, malnutrition, and trauma in the world's most vulnerable communities.
Now, you can be part of this humanitarian commitment at the first-ever MSF Bowling Challenge. Each pin you knock down represents a disease or crisis we're working to defeat in Sudan—malaria, measles, malnutrition, and the invisible wounds of violence. Your participation can help turn an evening of fun, into a lifeline for those in need.
ONE EVENING. ONE STRIKE AT A TIME.TOGETHER, WE CAN SAVE LIVES.
SUDAN: A HUMANITARIAN CRISIS IN 2026
Working in 8 of Sudan’s 18 states, MSF runs and supports hospitals and clinics, offering emergency care, surgeries, maternal and pediatric services, malnutrition treatment, vaccinations, and care for survivors of sexual violence. In 2026, the needs remain urgent. MSF needs your support.
MSF IN KENYA
Why join us?
For everyone
- Support Conflict-affected and Displaced Communities with practical, lifesaving medical care
- Participate in a fun, accessible, inclusive event
- Trial Experience: Evaluate the tournament's value firsthand.
Quick facts about Ebola and haemorrhagic fevers

Ebola is a disease group which includes the Ebola (also commonly referred to as Zaire), Sudan, and Bundibugyo viruses. They each have different virulence and fatality rates. Zaire is the most virulent and lethal, killing up to 90 per cent of people; Bundibugyo the least, with estimated case fatality rates between 25 and 40 per cent. Depending on the virus, Ebola can be found in parts of West and Central Africa (Zaire virus), DRC (Zaire and Bundibugyo viruses), Uganda (Sudan and Bundibugyo viruses), and Sudan (Sudan virus).

Once a case of haemorrhagic fever is confirmed, a swift response is vital. The needs of patients and affected communities must remain at the heart of the response, which can be defined by six main pillars : care and isolation of patients; tracing and follow up of patient contacts; raising community awareness of the disease such as how to prevent it and where to seek care; conducting safe burials; proactively detecting new cases; and supporting existing health structures.

Diagnosing haemorrhagic fever can be difficult, because early symptoms, such as fever and sore throat, are common to many illnesses, including malaria. For Ebola, it’s possible to use GeneXpert, a rapid test using cartridges in a machine, to diagnose Zaire virus. For Lassa fever, a rapid test is in development. A patient who has early symptoms of a haemorrhagic fever should isolated to prevent further risk of infection. Public health professionals should be notified, and a laboratory test must be carried out to confirm a diagnosis. Such tests are an extreme biohazard risk and should be conducted under maximum biological containment conditions.
There are now curative drugs available to treat the Zaire virus of Ebola, developed during the West Africa outbreak, and used during recent outbreaks in DRC. These drugs are not approved for other Ebola viruses. Antiviral medicines have also been used to treat Lassa fever. Otherwise, care involves maintaining a patient’s fluid and oxygen levels, nutrition support, providing fever and pain medication, and drugs to reduce vomiting and diarrhoea. Other diseases the patient may have, such as malaria or sepsis, should also be treated. Patients should be isolated to prevent infecting others. Psychological support should be provided to help patients and families.

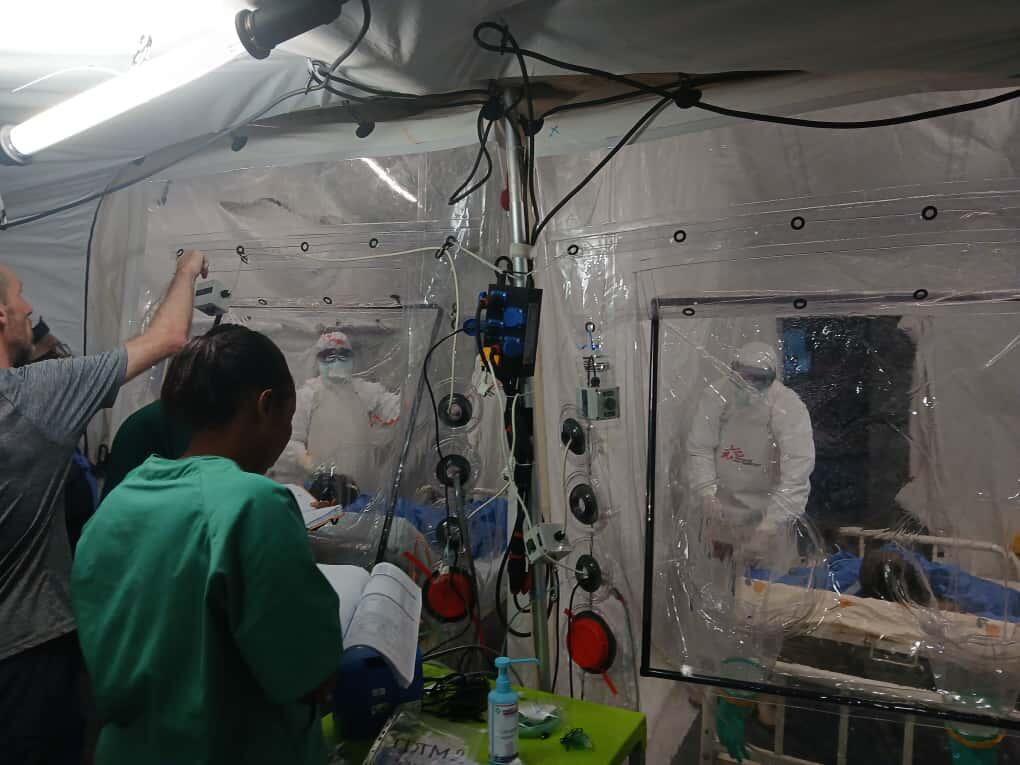
Human-to-human transmission occurs through contact with bodily fluids of an infected person or through surfaces contaminated with these fluids. Infection control in health centres is vital to reduce risks for other patients, caregivers, and health workers. Those caring for infected patients must wear personal protective equipment (PPE). Touching the body of an infected person who died can transmit the virus, so burial teams also use PPE, and safe burials must be carried out in a dignified manner for family members.

In the wake of the 2014-2016 West Africa Ebola epidemic, a vaccine was developed that can help control an outbreak of the Zaire Ebola virus. The vaccine, rVSV-ZEBOV, has been used during subsequent Ebola outbreaks in DRC, as part of the overall strategy to control epidemics. Ebola frontline workers and contacts of Ebola patients are those who are vaccinated on a priority basis during an outbreak.

Survivors often face stigma and are sometimes ostracised from their communities. This, and the trauma of having lived through such a deadly disease, often requires counselling. People may experience ongoing physical side-effects, such as joint pain, headaches and eye problems that require treatment and follow up. MSF established Ebola survivor centres in the three worst-affected countries after the West Africa epidemic.